
The thyroid gland is a butterfly-shaped gland located in the front of the neck just above the trachea in the adult human. Its pivotal role in regulating our body’s metabolism involves the secretion of two hormones: thyroxine (T4) and triiodothyronine (T3). In addition, it also secretes small amounts of biologically inactive reverse T3 and minute quantities of monoiodotyrosine(MIT) and diiodotyrosine(DIT) which are precursors of T3 and T4. Free T4 is the primary secretory product of the normal thyroid gland. Thyroid hormone synthesis and secretion are controlled by a negative feedback system involving thyrotropin-releasing hormone from the hypothalamus, TSH from the pituitary and thyroid hormones from the follicular cells of the thyroid glands.
Thyroid Hormone Symphony and Control
A sophisticated feedback system orchestrates thyroid hormone synthesis and secretion. The hypothalamus releases thyrotropin-releasing hormone, triggering the pituitary gland to release thyroid-stimulating hormone (TSH), which, in turn, prompts the thyroid to release its hormones. This helps maintain balance, ensuring the body’s metabolic equilibrium.
Pathological Insights: Hypothyroidism, Hyperthyroidism, and NTIs
The thyroid gland is at the heart of two primary pathological conditions: Hypothyroidism and Hyperthyroidism. Furthermore, nutritional deficiencies, acute illnesses, and chronic conditions collectively known as non-thyroidal illnesses (NTIs) can also impact thyroid function. In clinical settings, thyroid function tests, typically measured through immunoassay, play a crucial role in diagnosing thyroid disorders.
TSH as the First Line of Assessment
TSH stands as the initial benchmark for assessing thyroid hormone status. However, caution is warranted in its use in the presence of NTIs, pituitary disease, or when influenced by TSH-suppressing drugs.
FT4 as a Strategic Second-Line Test
Free T4 (FT4) assumes a second-line role, stepping in to investigate situations with TSH abnormalities or unreliable TSH measurements. Its focused application adds precision to the diagnostic process.
Free T4 and Ultrasensitive TSH are generally recommended in:
- Screening patients with suspected thyroid condition
- Newborn babies
- Screening patients with hyperthyroidism to differentiate between euthyroid and hyperthyroid
- Patients with secondary hyperthyroidism
- Monitoring treatment – thyroid replacement or suppression
FT3 for Targeted Diagnoses and Monitoring
Free T3 (FT3) is reserved for specific purposes such as diagnosing T3-toxicosis or monitoring T3 replacement therapy. Its selective use ensures accurate insights into thyroid function.
Free T3 and T4 screening is recommended in:
- Monitoring treatment – thyroid replacement or suppression
- Hospitalised patients, where patients may show symptoms of non-thyroidal illness
- Pregnant women with underlying thyroid condition
- Patients known to take certain drugs which will interfere with total T3 and T4 test results
- Elderly patients
Recovery Dynamics from NTIs
As patients recover from NTIs, the journey to normalcy begins. T4 concentrations take the lead in correction, succeeded by an elevation in T3 levels. Serum TSH may exhibit a transient rebound to higher concentrations for days or weeks before returning to a stabilized state.
Understanding these nuances in thyroid function testing not only aids in the precise diagnosis of disorders but also guides healthcare professionals in tailoring interventions. As the intricate web of thyroid health is unwoven, a clearer path to effective management and recovery emerges for individuals navigating these conditions.
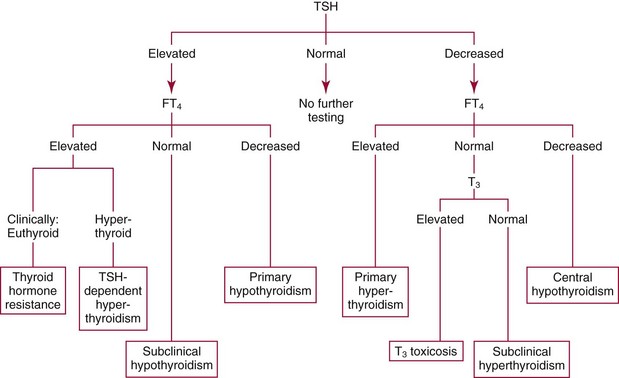
Suggested algorithm for the laboratory evaluation of thyroid function
 </p
</p
Patterns of Thyroid dysfunction
Primary hypothyroidism | Increased | Decreased | —- |
Sub Clinical Primary hypothyroidism | Increased | Normal | —- |
Primary hyperthyroidism | Decreased | Increased | T3 Increased |
T3 toxicosis | Decreased | Normal | T3 Increased |
Sub Clinical Primary hyperthyroidism | Decreased | Normal | T3 Normal |
Thyroid hormone resistance due to defects in the thyroid hormone receptor | Normal to increased | Increased | T3 Increased; rT3 Increased |
Thyroid hormone resistance due to defects in the thyroid hormone metabolism of T4 converted to T3 | Mildly increased | Increased | T3 decreased; rT3 Increased |
Thyroid hormone resistance due to defects in the thyroid hormone transport into cells | Normal to increased | Normal to decreased | T3 Increased; rT3 decreased |
Non Thyroidal Illness: A progressive spectrum of thyroid test result anomalies often accompanies NTIs in Euthyroid patients.
Hormone | Initial phase | Mid phase | Prolonged | Resolution |
TSH | Normal | Normal to Decreased | Decreased | Increases |
T4 | Normal | Normal to Decreased | Decreased | Increases |
T3 | Mildly decreased | Moderately decreased | Severely decreased | Increases |
Rt3 | Mildly Increased | Increased | Increased | Decreases |
Significance of Early Detection
Early diagnosis of thyroid disorders is vital for preventing complications, improving treatment outcomes, and preserving overall well-being. Timely intervention helps avoid hormonal imbalances, mitigates risks during pregnancy, and reduces the impact on mental health. Additionally, it minimizes cardiovascular effects and contributes to more cost-effective management. Regular thyroid function testing and awareness ensure early detection and effective control of thyroid disorders.
Transasia’s offerings for timely detection of Thyroid disorders
Transasia Bio-Medicals Ltd. provides advanced diagnostic solutions for early and accurate detection of thyroid conditions. Our range of ELISA screening kits encompasses ErbaLisa TSH, ErbaLisa Total T3 (tT3) and T4 (tT4), intended for qualitative measurement of thyroid hormones in the human serum.
Note: Allan-Herndon-Dudley syndrome: An X-linked syndrome caused by mutations in the SLC16A2 gene (locus: Xq13.2), which encodes a thyroid hormone transporter, and characterized by severe mental retardation, dysarthria, athetoid movements, muscle hypoplasia, and spastic paraplegia.
References:
- Tietz fundamentals of Clinical chemistry and molecular diagnostics. Chapter 42 Thyroid disorders.
